How Hormones Cause Melasma and Dark Spots — And What to Do About It
- Estrogen, progesterone, and androgens all influence melanin production directly.
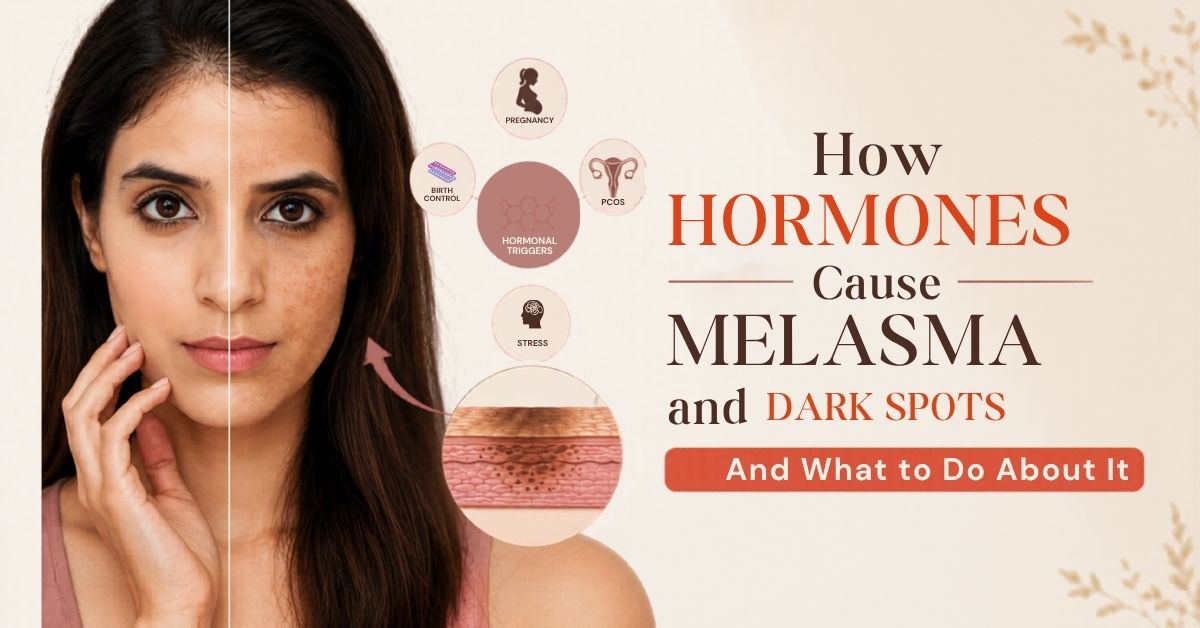
- PCOS, pregnancy, birth control, and menopause are the four most common hormonal pigmentation triggers in women.
- Melasma appears as butterfly-shaped patches on the forehead, cheeks, and upper lip — it is hormonal, not just sun damage.
- Topical creams alone will not clear hormonal pigmentation. The hormonal root cause has to be worked on at the same time.
- Internal rituals and dietary adjustments produce results that surface-only treatments cannot.
If your dark patches appeared during pregnancy, worsened when you started birth control, or seemed to come out of nowhere in your late thirties — your hormones are the most likely explanation.
Hormonal pigmentation is one of the most stubborn forms of skin discolouration. Women spend years trying every serum on the market, not realising that none of those products can touch the actual cause. The melanin keeps being produced because the hormonal signal telling it to produce has never been addressed.
Mansi Gulati’s approach starts with identifying which hormonal pattern is driving the problem — because PCOS skin looks different from pregnancy melasma, which looks different from post-menopause dark spots. The root cause shapes the treatment.
Why Hormones Trigger Melanin Production
Melanocytes — the skin cells that produce melanin — are sensitive to hormonal signals. Estrogen and progesterone both stimulate melanocyte activity. When these hormones fluctuate, as they do during pregnancy, menstrual cycles, or menopause, melanin production rises.
This is why women are significantly more prone to hormonal pigmentation than men. Male hormone levels are relatively stable across the lifespan. Female hormone levels go through consistent cycles — monthly, across pregnancies, and through perimenopause. Each of those cycles creates windows where melanin can spike.
Understanding the full picture of what causes pigmentation on the face is useful before focusing on the hormonal angle specifically.
Pregnancy and Melasma
Melasma during pregnancy is so common it has a nickname: the mask of pregnancy. It appears as brown or greyish patches across the forehead, cheeks, nose, and upper lip in a characteristic pattern.
During pregnancy, estrogen and progesterone levels rise sharply. Both hormones directly stimulate melanocyte-stimulating hormone (MSH), which tells the skin to produce more melanin. Combined with increased sun sensitivity that comes with pregnancy, the result is rapid pigmentation in the most exposed areas.
For many women, melasma fades after delivery as hormones normalise. For others — especially those who experience prolonged postpartum fluctuations or have a genetic predisposition — it persists for months or years. Postpartum skin recovery involves many of the same internal factors that drive pigmentation, and addressing them together makes a real difference.
PCOS and Skin Pigmentation
PCOS creates a different hormonal picture from pregnancy. The dominant issues here are elevated androgens and insulin resistance.
Elevated androgens stimulate skin inflammation, which drives Post-Inflammatory Hyperpigmentation — dark marks left behind by acne. Insulin resistance independently stimulates melanin production and can cause Acanthosis Nigricans, which appears as dark, velvety patches along the neck and jaw.
For women with PCOS, pigmentation on the face is often a combination of hormonally-driven melanin overproduction and inflammation-driven marks from recurring breakouts. Treating only the surface misses both underlying mechanisms entirely.
The gut-skin axis is particularly relevant here — insulin resistance affects gut health, gut health affects estrogen metabolism, and estrogen metabolism affects melanin. The liver and gut connection to pigmentation explains this cycle in detail.
Birth Control and Dark Spots
Oral contraceptive pills containing synthetic estrogen and progesterone are a well-documented melasma trigger. The synthetic estrogen stimulates melanocyte activity in the same way natural estrogen does during pregnancy — and this continues for as long as the pill is taken.
Women who develop pigmentation after starting the pill often don’t connect the two. They assume it’s sun damage or aging and keep using topical treatments that don’t work because the hormonal signal is still active every day. If you noticed dark patches appearing or worsening after starting oral contraceptives, this connection is worth discussing with your gynaecologist.
Menopause and the Estrogen Shift
Menopause creates a different pattern from what most people expect. While estrogen drops overall, the erratic fluctuations of perimenopause — the years leading up to the last period — can still actively drive new melanin production.
The drop in estrogen also reduces the skin’s collagen production and repair capacity. Marks that might have faded quickly in younger years now persist. Sun damage accumulated over decades becomes more visible. The skin is more vulnerable and less able to recover on its own.
Why Topical Treatments Fail for Hormonal Pigmentation
This is the frustrating reality most women hit eventually. Hydroquinone, vitamin C serums, kojic acid — all of these can reduce melanin at the skin surface. But while the hormonal signal is still active, the melanocytes keep producing. You fade what’s there, new pigmentation forms. The cycle continues.
Real improvement requires working on the hormonal root cause alongside any topical treatment. For PCOS-driven pigmentation, this means addressing insulin resistance and inflammation. For pregnancy melasma, it means supporting liver hormone clearance. For pill-related pigmentation, it may mean exploring non-hormonal alternatives.
What Mansi Recommends for Hormonal Pigmentation
The internal approach focuses on blood purification, liver support, and reducing inflammation — the same foundations that support overall hormonal balance.
Manjistha before bed is the first recommendation. As a blood purifier, it directly supports the liver’s ability to clear excess circulating hormones. Estrogen not properly cleared by the liver recirculates and continues to stimulate melanin. Manjistha helps break this cycle.
Amla with black pepper every morning provides Vitamin C support for liver function and antioxidant protection. For women with PCOS, Amla also supports insulin sensitivity over time.
Reducing sugar and refined carbohydrates is particularly important for PCOS-driven pigmentation. Both worsen insulin resistance, which amplifies the hormonal melanin signal.
For a structured programme that brings internal work, topical rituals, and face yoga together specifically for pigmentation, Mansi’s Pigmentation Correction Challenge is built for exactly this. The 28 Days Workshop is a broader skin health programme that works well alongside any targeted treatment.
Frequently Asked Questions
Can PCOS cause pigmentation on the face?
Yes. PCOS raises androgen levels and causes insulin resistance, both of which drive melanin overproduction. Women with PCOS often experience a combination of hormonally-triggered dark patches and Post-Inflammatory Hyperpigmentation from hormonal acne. Addressing insulin resistance and inflammation is essential alongside topical treatment.
Does melasma go away after pregnancy?
For many women, pregnancy melasma fades within a few months of delivery as hormone levels normalise. For others it persists, especially with a family history of melasma. Supporting the liver’s hormone-clearing function through Manjistha and Amla helps speed this process.
Can the contraceptive pill cause dark patches on the face?
Yes. Oral contraceptives containing synthetic estrogen are a documented melasma trigger. Women who notice pigmentation appearing or worsening after starting the pill should discuss non-hormonal alternatives with their gynaecologist.
Why is my skin getting darker during menopause?
The hormonal fluctuations of perimenopause can actively stimulate new melanin production. The decline in estrogen also reduces the skin’s repair capacity, making existing dark spots more visible and harder to clear.
Will vitamin C serums clear hormonal pigmentation?
Vitamin C serums can reduce surface melanin but cannot address the hormonal signal driving overproduction. Pairing topical treatment with internal support — Amla, Manjistha, dietary changes — produces significantly better and lasting results.